











































A Framework for Health Communication Across the HIV Treatment Continuum
Johns Hopkins Center for Communication Programs (Babalola, Van Lith, Mallalieu, Packman, Myers, Gurman, Figueroa); United States Agency for International Development (Ahanda, Harris)
"Communication approaches offer viable options for promoting relevant behaviors across the continuum."
This article introduces a conceptual framework, informed by a social-ecological perspective, to guide the development of health communication interventions that have been shown to impact behaviours across the HIV treatment continuum in low- and medium-income countries. Consistent with the World Health Organization (WHO)'s guidelines on HIV treatment and the current focus on "test and treat", the framework includes: (i) HIV testing and counseling, (ii) linkage to care and treatment, and (iii) adherence to antiretroviral therapy (ART).
The authors define social and behavioural change communication (SBCC) or health communication as "a process with multiple functions, including informing people about health-protective behaviors, persuading or motivating people to adopt health-protective behaviors, building social connections, and fostering an enabling environment....Health communication can influence behaviors along the HIV continuum irrespective of where the behavior occurs along the social–ecological model" by, for example, strengthening self-efficacy and motivating individuals to get tested and obtain their results, empowering HIV counselors to better engage with their clients and address their ART-related concerns to successfully link them to HIV care, encouraging adherence and retention to achieve viral suppression, and strengthening social support for people living with HIV (PLHIV) and addressing stigma, a key barrier to ART initiation and adherence.
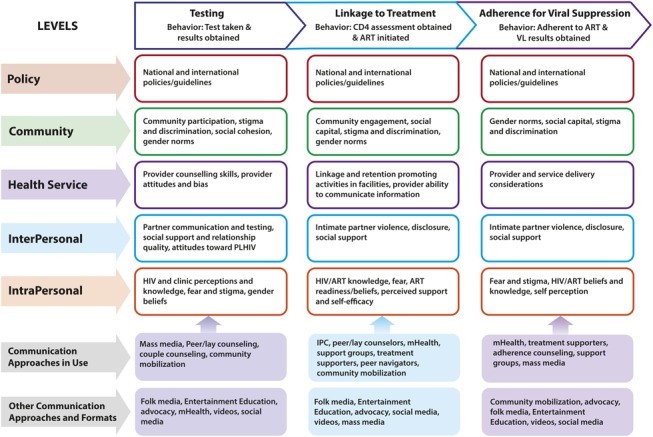
The conceptual framework and evidence presented highlight areas across the continuum where health communication can significantly impact treatment outcomes to reach the Joint United Nations Programme on HIV/AIDS (UNAIDS) 90-90-90 goals [that 90% of all PLHIV know their status, 90% of all diagnosed PLHIV receive ART, and 90% of all persons receiving ART achieve viral suppression] by strategically addressing key behavioural determinants. The top row in the model presents the desired behaviours at each of the 3 key stages of the continuum. The determinants of behaviour operate at multiple levels. From top to bottom, these levels include national policy, community, services, interpersonal, and intrapersonal levels. At each level and for each behaviour, determinants include both facilitators and barriers, with communication interventions designed to focus on specific determinants presented in the model. The last row of the model presents health communication interventions found in the articles reviewed, as well as the suggested approaches that address the identified determinants (see Supplemental Digital Content 1 for more information on the included interventions).
The first step in the continuum of ensuring that 90% of PLHIV know their HIV status centres on HIV testing and counseling (HTC). As countries move to test and treat policies, reframing HTC as an opportunity for early diagnosis and treatment to prevent illness and transmission is needed, the authors argue here. They explore the determinants at each level of their conceptual framework; for instance, at the intrapersonal level, studies have emphasised the importance of psychosocial (ideational) determinants, including cognitive (knowledge, beliefs, and attitudes), emotional, and social interaction determinants. Their review of the literature shows that health communication interventions that have successfully addressed these and other determinants outlined include those implemented at the intrapersonal level (e.g., the use of mass media to promote HTC) and the interpersonal level (e.g., peer support and counseling for male partners of pregnant women and couple-oriented counseling). Successful approaches at the community level include use of existing socially accepted community-based infrastructure (e.g., churches) and use of lay counselors to build trust and acceptability, mitigate stigma, and serve as an acceptable entry point into the HIV continuum. Other community-level interventions, including availability of counseling resources in the community and the provision of community-based testing services with or without peer or lay counselors (including door-to-door, self-testing, mobile-testing, workplace-based, school-based, church-based, etc.) have been found to increase testing.
Linkage to care and treatment, including pre-ART care and treatment initiation, will ideally immediately follow an HIV-positive diagnosis. Often, however, clients choose to delay seeking care or initiating treatment after diagnosis. Again, here, determinants at each level are outlined in the paper. Successful interventions using various counseling and psychosocial support strategies have been documented, including: peer support, information, and education; identifying and addressing clients' barriers to service use; and providing help with appointment coordination. Training counselors on post-test counseling, provision of social and psychological support, mobile health reminders, patient-selected care buddies, and peer navigators have been found to increase linkage to care and treatment. Successful interventions at the health services level highlight issues such as the importance of coordination between facility-based and community-based activities by health personnel. At the community level, support groups and strong networks, where home-based care organisations, community volunteers, and HIV education programs are in place, reduce stigma and discrimination, improve linkage and retention in pre-ART care, and increase early ART initiation. Interventions engaging traditional practitioners and faith healers yielded mixed results.
Third, the determinants of antiretroviral (ARV) treatment adherence have been well documented and span across the social–ecological model; to cite only one example from the paper: "Social capital and community engagement in the care and support of PLHIV may...foster adherence." Most interventions using elements of health communication to promote adherence targeted determinants operating at the intrapersonal level. For example, mHealth programmes using short message service (SMS/text) or interactive voice responses implemented as a stand-alone intervention or as part of a more comprehensive strategy remind patients to take their medications and provide remote psychosocial support. Interventions have often but not always been effective. At the interpersonal level, treatment supporters or companion or buddy strategies are designed to strengthen social connection by facilitating disclosure and providing one-on-one adherence and psychosocial support. Results have been mixed. At the health services level, repeated adherence counseling has shown promising results for adherence and viral suppression. Effective interventions at the community level include, for example, peer adherence support groups or adherence clubs, although 1 study did not demonstrate a positive result and attributed inadequate facilitation skills of the lay health workers.
In reflecting on these findings, the authors assert that the evidence shows that interventions that include health communication components have been successful in addressing the determinants of the behaviours along the HIV treatment continuum. "Most interventions reviewed relied on interpersonal communication through peers, community support groups, and home visits. This mode of communication through social networks is of utmost importance, as it relies on relationships and social bonds to help HIV-positive individuals navigate hurdles across the continuum. Counseling through community volunteers and lay counselors is also an effective approach, specifically when counselors received training on interpersonal communication skills for post-test counseling and psychological support for disclosure and treatment uptake. Furthermore, mHealth interventions promoting linkage to treatment or adherence have yielded promising results. Limited evidence in the literature reviewed was found on the use of multimedia health communication campaigns that combine 2 or more approaches and delivery channels, including, interpersonal communication, mass media, educational entertainment, folk media, mobile devices, social media, and advocacy to promote behaviors along the continuum."
As test and treat rolls out, the authors argue, multifaceted health communication approaches will be critical in successfully addressing the determinants of testing, early initiation of ART, and adherence. "The complexity of the behaviors and determinants required to fulfill the 90-90-90 goals requires a combination of communication approaches for synergistic effects." They provide several examples. To cite only one: ART literacy, to better understand the negative association between CD4 (high is good) and viral load (high is bad) and appreciate the need for repeated viral load testing, could be successfully addressed by combining interpersonal approaches at the facility and community levels with mass media, providing the added benefit of disseminating consistent information to multiple audiences at a large scale and in a cost-effective manner.
In conclusion: "Strategic, multiphase, multifacet communication interventions are needed to inform individuals about services, remove misconceptions about testing and treatment, further reduce stigma, improve couple's communication and support, and help communities create supportive environments where PLHIV can successfully manage HIV and enjoy a quality life."
Journal of Acquired Immune Deficiency Syndromes, Volume 74, Supplement 1, January 1 2017.
- Log in to post comments