











































Time for Action: Towards an Intersectional Gender Approach to COVID-19 Vaccine Development and Deployment that Leaves No One Behind
World Health Organization, or WHO (Heidari, Goodman); University of Newcastle (Durrheim); member of WHO Strategic Advisory Group of Experts (SAGE) COVID-19 Vaccines Working Group (Durrheim, Faden, Kochhar, MacDonald, Olayinka); Johns Hopkins University (Faden); Global Healthcare Consulting (Kochhar); University of Washington (Kochhar); Dalhousie University Faculty of Medicine (MacDonald); member of WHO SAGE (MacDonald, Olayinka); Public Health Institute/STAR (Olayinka)
"[A] gender-transformative approach has the potential to optimise programmes and ensure equitable access to COVID-19 vaccines."
Sex and gender intersect with variables such as age, race and ethnicity, and other health conditions, resulting in differential risks and outcomes of COVID-19. For example, sex-based differences in vaccine-induced immune response and adverse events may influence vaccine acceptance, access, and uptake, which are also highly gendered. Hence, as the authors of this commentary argue, it is imperative that sex and gender be considered alongside other intersecting dimensions when developing and deploying COVID-19 vaccines. With a view to advocating for meaningful engagement of the expertise and leadership of women in all scientific research, policymaking, and programmatic decision-making processes, this article provides a critical review of the role of sex and gender dimensions in COVID-19 - from vaccine development to delivery.
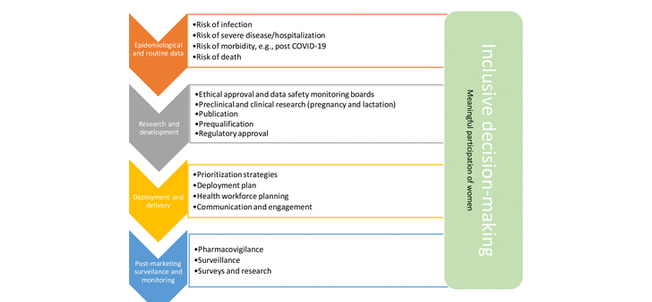
Specifically, the article offers six recommended actions for incorporating an intersectional gender lens in COVID-19 vaccine development and deployment efforts:
- Routinely collect, analyse, and report epidemiological data by sex and age to inform vaccination strategies - Data on testing, hospitalisation, intensive care unit (ICU) admission, and the post-COVID-19 condition are rarely available by sex, minority group status, and other indicators; we need these data to understand which groups are at greater risk and why and to inform targeted interventions in light of limited capacity and resources.
- Design COVID-19 vaccine studies to adequately capture sex and gender differences in safety, efficacy, and effectiveness of vaccines - Vaccine trials are rarely designed to capture sex or gender differences, seldom report outcome data by sex, and inadequately examine implications in terms of gender. To successfully enrol and retain sufficient numbers of women and men in vaccine trials, a gender lens must be applied to every aspect of trial design. Ethics committees and data safety and monitoring boards must require consideration of sex and gender in study protocols and review these dimensions in interim analyses and monitoring.
- Generate data on safety, efficacy, and effectiveness of vaccines in pregnant women and lactating women at an early stage - Data on the safety and efficacy of COVID-19 vaccines during pregnancy and lactation are very limited. Pregnant women have historically been excluded from clinical trials, and yet it is critical that pregnant and lactating women be included in appropriately designed vaccine trials to generate sufficient and timely evidence about the safety of vaccines on pregnancy outcomes and to assess immune responses to vaccination in pregnant women.
- Ensure that COVID-19 prioritisation strategies and deployment plans are gender responsive and mindful of gender-related barriers to immunisation - In light of the gender gaps and biases in available data, national prioritisation decisions must be transparent about the rationale and the evidence on which groups are prioritised. At the same time, data collection capacity and monitoring must be strengthened. Similarly, vaccine deployment plans need to be designed with gender and other equity concerns in mind. Issues such as provider attitudes, communication, education and health literacy, autonomy and agency, access and control over resources, and gender-based violence come into play during COVID-19 vaccine deployment and may create gender-related barriers to immunisation. Furthermore, the well-being and resilience of health and social workers, most of whom are women, are paramount during the pandemic and vaccination roll-out.
- Collect disaggregated data regarding to capture potential differential effects and uptake - Vaccine hesitancy and other factors related to confidence in and acceptability of COVID-19 vaccines are gendered and can be negatively influenced by harmful gender norms, beliefs, and expectations. Differences between women and men in these domains underscore the necessity for pharmacovigilance, surveillance, and monitoring systems to collect, analyse, and report data by sex and other indicators to identify or rule out discrepancies in vaccine safety and experience of adverse events, which can feed vaccine resistance. Qualitative studies (including ethnographic research) may shed further light on contextual gender dimensions and increase understanding of underlying causes for and consequences of vaccine hesitancy. Accordingly, it is important to consider gender and equity dimensions when developing communication and advocacy materials: how information on vaccination and vaccine safety is communicated and by whom, the languages used, who is portrayed in the material and how, whom the materials reach and how they are perceived, and the way information is distributed and disseminated (as well as the choice and use of social media and the messaging).
- Foster equal participation of women in decision-making at all levels to support successful vaccine implementation - Gender imbalances in the management and decision-making positions of the health sector must be addressed, and decision-making processes at national, subnational, or international levels must ensure women, especially women health workers, are engaged and involved in decisions and in the development of policies and programmes. International COVID-19 vaccine governance structures and regional and national committees related to vaccination need to be gender balanced and inclusive.
In conclusion: "The lessons learnt from COVID-19 vaccines are relevant for future research and development of other vaccines. Applying an intersectional gender lens at each step of the process will help identify potential sex differences, and gender-related inequities, and support tailored vaccination programmes that can effectively respond to the diverse needs and experiences of women, men and non-binary persons, thereby ensuring vaccination of 'everyone, everywhere'."
BMJ Global Health 2021;6:e006854. http://dx.doi.org/10.1136/bmjgh-2021-006854
- Log in to post comments