











































How to Increase and Maintain High Immunization Coverage: Vaccination Demand Resilience (VDR) Framework
University of North Carolina at Chapel Hill (Ozawa, Yemeke, Lee); Johns Hopkins Bloomberg School of Public Health (Schuh); London School of Hygiene and Tropical Medicine (Nakamura); Nagasaki University (Nakamura); Dalhousie University (MacDonald)
"Fostering vaccination resilience requires understanding the dynamics of vaccination demand and implementing appropriate interventions to increase and maintain vaccination demand."
Country immunisation programmes have been facing challenges to reach and maintain vaccine coverage targets, overcome access disparities, and ultimately avert deaths from vaccine-preventable diseases. Demand-side barriers have increasingly come to the forefront of challenges in building vaccination resilience, which refers to immunisation systems that are able to withstand major shocks and disruptions. Beyond increasing vaccination coverage, resilience is about growing and maintaining high coverage over time across various vaccines and age groups, and having communities strongly support routine immunisations. To help conceptualise vaccination demand and build resilience, the framework presented in this article captures the multiple factors that can impact individual and community vaccine acceptance/demand; it can be used by immunisation programme managers and policymakers to improve and sustain vaccination uptake.
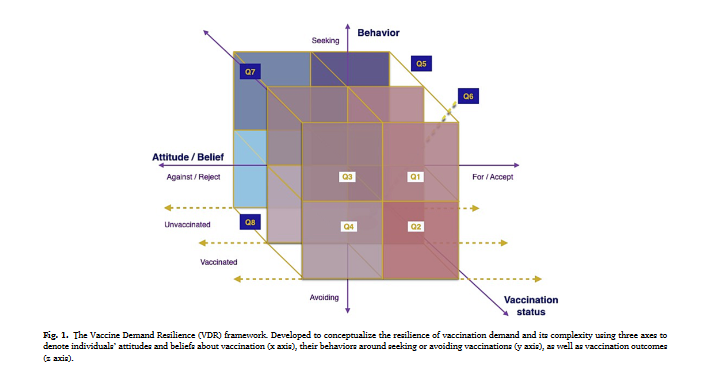
Developed following a literature review on vaccination demand and experts' feedback, the Vaccination Demand Resilience (VDR) framework was built based on three analytical dimensions: (i) an attitudinal/belief axis, ranging from the extent to which an individual's attitude/belief in vaccination is strongly positive and accepting, versus negative and rejecting; (ii) a behavioural axis, ranging from active seeking of vaccination services to active avoiding of vaccination services; and (iii) an outcome of vaccination status axis that captures outcome measures such as immunisation coverage estimates, ranging from completely vaccinated to completely unvaccinated status.
This framework can be applied across the age span from infancy to older adults by considering whose behaviours, attitudes/beliefs, and vaccination status is most relevant to each vaccination. For example, for childhood vaccines, mothers', fathers', or caregivers' attitudes and beliefs about vaccinations and their vaccination-seeking behaviours would impact children's vaccination status. This framework could also be applied for vaccine-specific or dose-specific differences in individuals' attitudes and beliefs, behaviours, and vaccination outcomes.
The three axes generated eight quadrants that can explain people's levels of vaccination demand. Each quadrant represents individuals' attitudes and beliefs about vaccinations, vaccination behaviours, and vaccination status, generating combinations that demonstrate their level of resilience toward vaccination demand. For example, quadrant 1 (Q1) represents individuals who fully accept the benefits of vaccinations, actively seek vaccinations, and are vaccinated. On the other hand, individuals in quadrant 8 (Q8) reject the benefits of vaccination, actively avoid vaccinations, and remain unvaccinated. The quadrants in between (Q2-Q7) demonstrate the challenge of vaccination demand resilience, where mismatches between individuals' attitudes and beliefs, behaviours, and vaccination outcomes can challenge individuals' vaccination demand resilience. Incongruence between individuals' attitudes and beliefs, vaccination behaviour, and vaccination status could be altered by interventions involving changes in policies, programmes, or practices.
The paper explores four scenarios, each with several examples, to demonstrate different interventions that could move people across quadrants and build vaccination resilience.
- Interventions to change vaccination attitudes and beliefs: These interventions may include information, education on media literacy and ability to recognise and resist disinformation, and communication interventions that aim to change negative attitudes and beliefs about vaccination through improved knowledge and awareness about vaccines. Such interventions can be tailored to the specific reasons and context behind lack of vaccine acceptance, including a focus on particular vaccines.
- Interventions to change vaccination-seeking behaviour: Incentive programmes and reminder-recall interventions are examples of such interventions to facilitate or induce vaccination seeking by increasing convenience and affordability.
- Interventions to change vaccination status: Policymakers can utilise vaccination mandates or school vaccination requirements to influence vaccination status without necessarily changing the attitudes and beliefs of individuals who may otherwise be unvaccinated in the absence of these policies. While some mandates include provision for mandatory counselling by health officials whereby individuals claiming exemptions have to receive educational information about vaccines, they have not yet been shown to change attitudes and beliefs.
- Interventions to strengthen patient-provider communication: Healthcare provider recommendations are one of the strongest predictors of vaccinations. Such health recommendations should be respectful of potential recipients' lived experiences, be culturally informed, and be sensitive to previous health system rebuffs. Healthcare provider discrimination could be harmful, where providers dismissing families refusing vaccines can have legal, ethical, and negative population health and trust implications.
Per the researchers, there were three key lessons in the development of the VDR framework:
- A framework that aids in describing the population dynamics of those individual-level decisions further supports the understanding that vaccination decision-making is complex and dynamic. Existing methods to understand vaccine acceptance and uptake such as the 3Cs (complacence, confidence, convenience), 5 Cs (confidence, complacency, constraints, collective response, calculation), 7 Cs (confidence, complacency, constraints, collective response, calculation, compliance, conspiracy), and 5As (access, affordability, awareness, activation, acceptance) and the Behavioural and Social Drivers models are limited for exploring the complexity of this decision-making process. The VDR framework not only identifies the degree to which individuals may be hesitant or opposed to vaccination, but also the resilience of vaccination decisions among people who are vaccinated to maintain immunisation coverage.
- As the VDR framework components are interrelated and decision-making is dynamic, looking at them solo can obscure one's understanding of why individuals may or may not vaccinate. For vaccination demand to be resilient, there needs to be "perfect" positive congruity of attitudes/beliefs, behaviours, and vaccination outcomes (Q1). Incongruence exists across the three axes in 6 of the 8 quadrants. Further, attitudes and behaviours that exhibit as hesitancy, passivity, and complacency toward vaccination likely exist along a spectrum, and individuals and populations can occupy different spaces within quadrants and along the axes. A combination of interventions, such as those outlined in the scenario examples, will be necessary to target the multiple dimensions of vaccination demand.
- Simply understanding one dimension - individuals' attitudes/beliefs, behaviours, or vaccination status - may not be a good way to predict future vaccination outcomes. For instance, only examining vaccination status is insufficient, as some vaccinated individuals may need additional reassurance to continue to demand vaccinations in the future. It is essential to listen to individuals and communities to understand the contextual factors and drivers of their vaccination demand. Vaccination demand is also fluid, where demand may be different from vaccine to vaccine and could change over time, requiring flexible and context-specific interventions.
In conclusion, the VDR framework "presents a mechanism to understand how different individuals within a community may make decisions about vaccination....It emphasizes the need for further data to translate global guidance to country-specific or community-specific situations to improve vaccination demand....By highlighting the population's views on vaccines in a systematic way, the VDR framework can provide a differentiated lens for program managers and policy makers to more thoughtfully consider interventions and policies to improve vaccination resilience."
- Log in to post comments